
The correct answer is (c) I, II and III.
Quick Breakdown:
- Correct for ventricular aneurysm post-MI:
I. Paradoxical (dyskinetic) impulse on chest wall
II. Persistent ST elevation on ECG
III. Unusual bulge from cardiac silhouette on X-ray - Not correct / unrelated: IV. Pulsus paradoxus (this is classically associated with cardiac tamponade or pericardial effusion, not ventricular aneurysm).
Blog Post: Diagnosing Post-MI Ventricular Aneurysm – Key Clinical & Imaging Clues
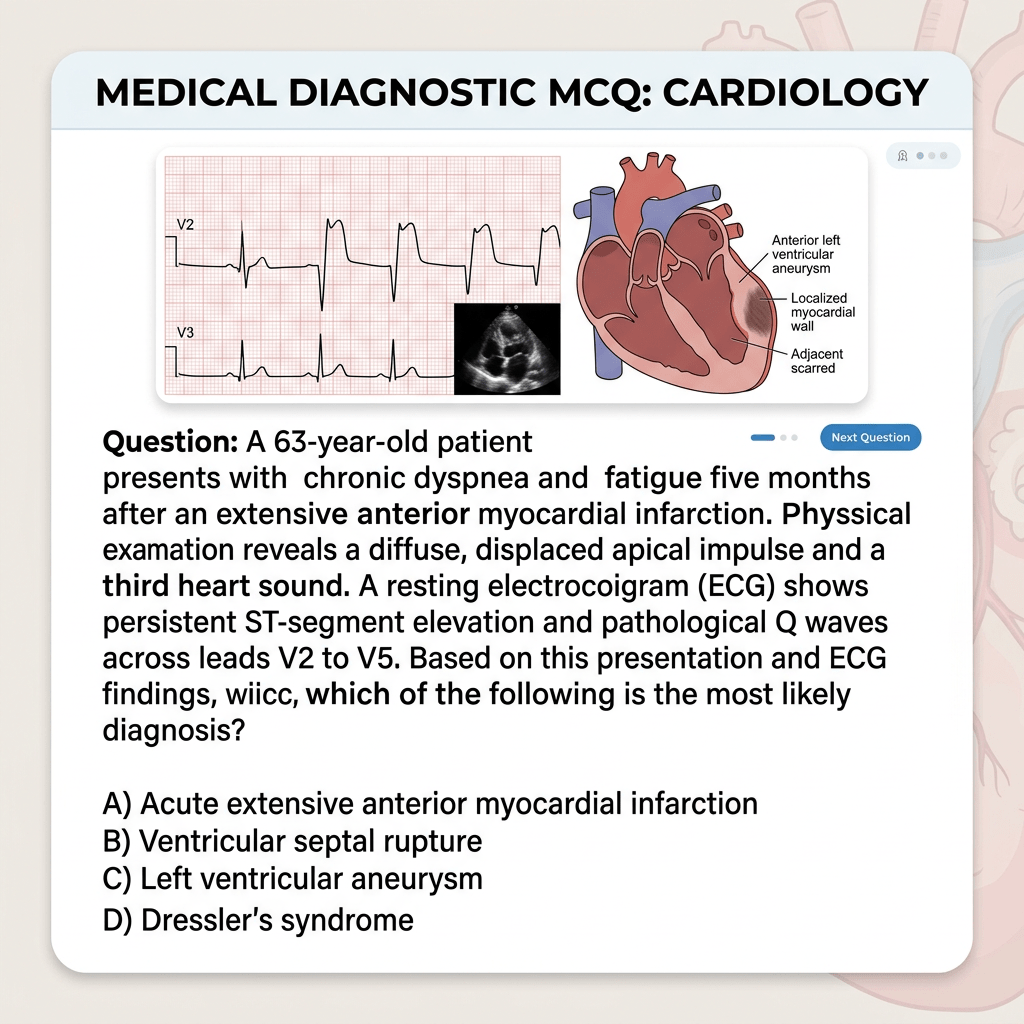
Left ventricular aneurysm is a serious mechanical complication following a transmural myocardial infarction (especially anterior wall). It occurs when the infarcted myocardium thins and bulges outward, leading to dyskinetic or akinetic segments. Early recognition is crucial to prevent complications like heart failure, ventricular arrhythmias, thromboembolism, or rupture.
Classic Diagnostic Features
I. Paradoxical Impulse on Chest Wall
On palpation, you may feel a sustained, dyskinetic (paradoxical) bulge or impulse, often medial and superior to the normal apical impulse. This occurs because the aneurysmal segment moves outward during systole while the rest of the ventricle contracts inward. It is a valuable bedside clue, best appreciated in the left lateral position or with bimanual palpation.
II. Persistent ST Elevation on ECG
One of the most characteristic findings: ST-segment elevation that persists beyond 2–4 weeks after the acute MI (instead of resolving). It is usually seen in the infarct-related leads (e.g., anterior leads V1–V4) along with deep Q waves. This ECG pattern has reasonable specificity for aneurysm formation and correlates with paradoxical wall motion on echo.
III. Unusual Bulge from Cardiac Silhouette on Chest X-ray
A classic radiographic sign is a localized bulge or abnormal contour along the left heart border (often anterolateral or apical). This may appear as a well-circumscribed opacity projecting beyond the normal cardiac outline. While not always present in small aneurysms, it is highly suggestive when seen.
IV. Pulsus Paradoxus – Why It’s NOT a Feature
Pulsus paradoxus (exaggerated drop in systolic BP >10 mmHg during inspiration) results from exaggerated ventricular interdependence, most commonly in pericardial tamponade. It is not a feature of ventricular aneurysm and does not help in its diagnosis.
Why Option (c) is Correct
Statements I, II, and III align directly with established clinical, electrocardiographic, and radiographic signs of post-MI ventricular aneurysm. Statement IV belongs to a different differential (e.g., tamponade, severe asthma, constrictive pericarditis).
Modern Confirmation & Management Pearls
- Gold standard: Echocardiography (or cardiac MRI) to confirm dyskinetic segment with wide neck (true aneurysm).
- Complications to watch for: Congestive heart failure, mural thrombus, ventricular tachycardia.
- Treatment: Medical optimization, anticoagulation if thrombus present, and surgical repair (aneurysmectomy ± CABG) in selected symptomatic cases.
Bedside examination and basic investigations like ECG and chest X-ray still play a vital role in suspecting this diagnosis, especially in resource-limited settings. Always correlate with echo for definitive confirmation.

Leave a comment