
The correct answer is (d) They typically appear more than 3 weeks after onset of other clinical manifestations.
Quick Breakdown:
- (a) Incorrect — Subcutaneous nodules are typically found over extensor surfaces of joints, bony prominences (elbows, knees, wrists, occiput, spine), not flexor aspects.
- (b) Incorrect — They are painless and non-tender (firm, mobile).
- (c) Incorrect — Usual size is 0.5–2 cm (often smaller, a few mm to 2 cm), not 3–5 cm.
- (d) Correct — They usually appear late (several weeks, often 4–6 weeks or >3 weeks after other manifestations) and are strongly associated with carditis.
Subcutaneous Nodules in Acute Rheumatic Fever – The “Late Comer” Major Criterion
Subcutaneous nodules remain one of the five major Jones criteria for diagnosing acute rheumatic fever (ARF), yet they are relatively uncommon (occurring in <10% of cases, sometimes quoted 0–10% or even <2%). They are highly specific when present and almost always signal severe carditis. Understanding their exact characteristics helps avoid diagnostic pitfalls.
Classic Features of Rheumatic Subcutaneous Nodules
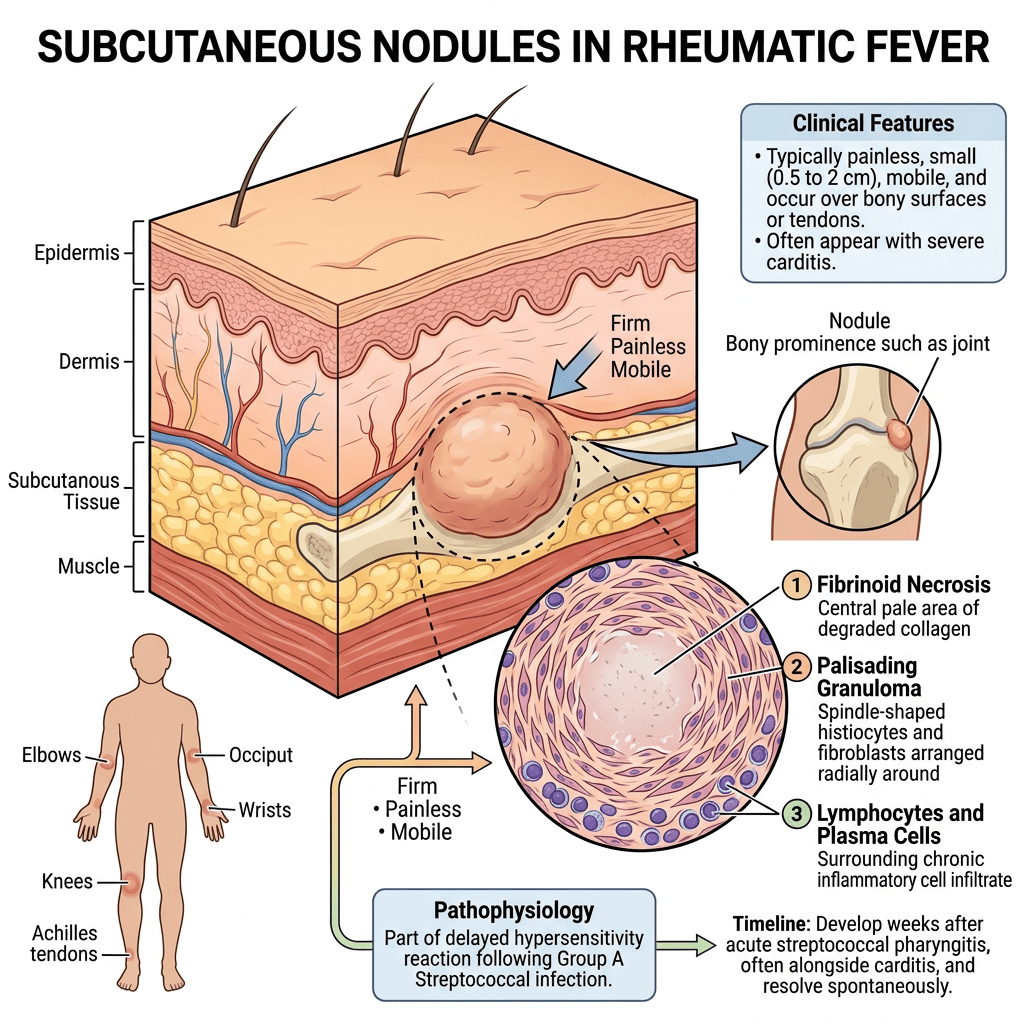
- Painless & Non-tender: Firm, mobile, skin-colored or slightly erythematous nodules. They do not hurt on palpation (unlike erythema nodosum or rheumatoid nodules in some contexts).
- Location: Over extensor surfaces and bony prominences — elbows, knees, wrists, ankles, occiput, spinous processes of vertebrae, and sometimes scalp. Not flexor surfaces.
- Size: Small — typically 0.5 to 2 cm in diameter (rarely larger).
- Number & Duration: Often multiple (can be few to dozens); they last days to weeks (sometimes up to a month or more) and resolve spontaneously.
- Timing — The key point: They are a late manifestation. They typically appear several weeks (commonly 4–6 weeks) after the onset of other features like arthritis, carditis, or fever. They are rarely the presenting sign and almost never occur in isolation.
Why Option (d) is Correct
This delayed appearance correlates with the autoimmune pathogenesis of ARF. By the time nodules develop, patients usually already have established carditis, which is why their presence should prompt urgent cardiac evaluation (echo is mandatory).
Comparison with Mimics
| Feature | Rheumatic Subcutaneous Nodules | Erythema Nodosum / Other Nodules |
|---|---|---|
| Tenderness | Painless | Often tender |
| Location | Extensor / bony prominences | Shins (erythema nodosum) |
| Size | 0.5–2 cm | Variable, often larger |
| Timing in ARF | Late (>3 weeks) | Not specific |
| Association | Severe carditis | Other causes |
Clinical Take-Home Messages
- Always search carefully for these nodules in suspected ARF — they are easy to miss if you don’t palpate extensor surfaces and scalp.
- Their presence upgrades the diagnosis and indicates higher risk of chronic rheumatic heart disease.
- Treatment is the same as for other ARF manifestations: anti-inflammatory therapy (aspirin/steroids), penicillin prophylaxis, and cardiac management.
Subcutaneous nodules may be rare, but when you spot them in the right context, they are diagnostically powerful. Late appearance is their hallmark — never dismiss a patient with carditis just because nodules are absent early on.
Keep examining thoroughly! Have you ever diagnosed ARF primarily because of subcutaneous nodules? Share your experience.

Leave a comment